1. Introduction
LVH in increased LV load is risk for early systolic HF. In increased LV afterload, as found in arterial hypertension, coarctation or aortic stenosis, relative effects of chronic late compared to early afterload on LV potential energy, stroke work and pressure-volume loop’s area, a parameter for LV O₂ demand with effective LV work are not defined in terms of earlier development systolic LV dysfunction (SD) with HF
| [1] | Lam YY, Kaya MG, Li W, Gatzoulis MA, et al. Effect of Chronic Afterload Increase on Left Ventricular Myocardial Function in Patients With Congenital Left-Sided Obstructive Lesions Am J Cardiol 2007; 99: 1582–1587. |
| [2] | Nozawa T, Yashumura Y, Futaka S, Tanaka N, Igarashi Y, et al. Relation between oxygen consumption and pressure-volume area of in situ dog heart. Am J Physiol 1987; 253: H31-H40. |
| [6] | Burkhoff D, Yue DT, Oikawa RY, Franz MR, Schaefer J, Sagawa K. Influence of ventricular contractility on non-work-related myocardial oxygen consumption. Heart and Vessels, 1987; 3: 66–72. |
| [12] | Suga H, Hisano R, Hirata S, Hayashi T, Yamada O, Ninomiya I. Heart rate-independent energetics and systolic pressure-volume area in dog heart. Am J Physiol. 1983 Feb; 244(2): H206-14. https://doi.org/10.1152/ajpheart.1983.244.2.H206 |
| [15] | Starling MR, Mancini GB, Montgomery DG, Gross MD. Relation between maximum time-varying elastance pressure-volume areas and myocardial oxygen consumption in dogs. Circulation 1991; Jan; 98(1): 304-14. https://doi.org/10.1161/01.cir.83.1.304 |
| [18] | Popevska S et al. Different left ventricular remodeling between descending thoracic vs. ascending aorta banding in porcine model. Abstract presentation ESCVS 2019 Groningen NL. published in Journal of Cardiovascular Surgery 2019; Vol 60, Suppl. 1 to No3.: 401, 56. |
| [22] | Abou Ezzeddine OF, Kemp BJ, Borlaug BA et al, Myocardial Energetics in Heart Failure. Circ Heart Fail. 2019; 12: e006240. https://doi.org/10.1161/CIRCHEARTFAILURE.119.006240 |
[1, 2, 6, 12, 15, 18, 22]
.
Diastolic LV function can deteriorate when the potential LV energy has been converted and used to generate wasted LV work, thus presenting inefficient contractions. This eventually results in development of earlier SD.
ACE inhibition increases LV O₂ consumption, reduces O₂ demand and improves LV stiffness, from stroke work with effective work, and novel antihypertensive treatments, with dapagliflozines
| [3] | Loke KE, Messina EJ, Shesely EG. Et al. Potential role of eNOS in the therapeutic control of myocardial oxygen consumption by ACE inhibitors and amlodipine. Cardiovascular research 2001; 49(1), 86-93. https://doi.org/10.1016/S0008-6363(00)00196-6 |
[3]
. This is important for adequate treatments of HTA and AS patients, having increased LV load.
LV pressure-volume loop’s area is relevant for assessing diastolic LV dysfunction, in different cardiovascular conditions in early SD. This includes the LV contractility in afterload associated hypertrophy, as well as the LV myocardium O₂ consumption. It has been of relevance to assess SD, in LVH remodeling
| [1] | Lam YY, Kaya MG, Li W, Gatzoulis MA, et al. Effect of Chronic Afterload Increase on Left Ventricular Myocardial Function in Patients With Congenital Left-Sided Obstructive Lesions Am J Cardiol 2007; 99: 1582–1587. |
| [4] | Suga H, Hayashi T, Shirahata M. Ventricular systolic pressure-volume area as predictor of cardiac oxygen consumption. Am J Physiol. 1981 Jan; 240(1): H39-44. https://doi.org/10.1152/ajpheart.1981.240.1.H39 |
| [5] | Burkhoff D, Sagawa K. Ventricular efficiency predicted by an analytical model. The American Journal of Physiology, 1986; 250(6): R1021–R1027. |
| [7] | Suga H, Hisano R, Goto Y, Yamada O, Igarashi Y. Effect of positive inotropic agents on the relation between oxygen consumption and systolic pressure volume area in canine left ventricle. Circulation Research, 1983; 32(3): 306–318. |
| [8] | Suga BH, Sagawa K. Instantaneous Pressure-Volume Relationships and Their Ratio in the Excised, Supported Canine Left Ventricle. Circulation Research, 1974; 35: 117–126. |
| [9] | Suga H, Sagawa K, Shoukas AA. Load independence of the instantaneous pressure-volume ratio of the canine left ventricle and effects of epinephrine and heart rate on the ratio. Circ Res. 1973; 32(3): 314-322. https://doi.org/10.1161/01.res.32.3.314 |
| [10] | Hansson NH, Sörensen J, Harms HJ, Kim WY, Nielsen R, Tolbod LP, et al. Myocardial Oxygen Consumption and Efficiency in Aortic Valve Stenosis Patients With and Without Heart Failure. J Am Heart Assoc. 2017 Feb 6; 6(2): e004810. https://doi.org/10.1161/JAHA.116.004810 |
| [11] | Suga H, Goto Y, Yasumura Y, Nozawa T, Futaki S, Tanaka N, Uenishi M. Oxygen-saving effect of negative work in dog left ventricle. American Journal of Physiology-Heart and Circulatory Physiology, 1988; 254(1), H34–H44. https://doi.org/10.1152/ajpheart.1988.254.1.H34 |
| [12] | Suga H, Hisano R, Hirata S, Hayashi T, Yamada O, Ninomiya I. Heart rate-independent energetics and systolic pressure-volume area in dog heart. Am J Physiol. 1983 Feb; 244(2): H206-14. https://doi.org/10.1152/ajpheart.1983.244.2.H206 |
| [13] | Nozawa T, Yasumura Y, Futaki S, Tanaka N, Uenishi M, Suga H. Efficiency of energy transfer from pressure-volume area to external mechanical work increases with contractile state and decreases with afterload in the left ventricle of the anesthetized closed-chest dog. Circulation, 1988; 77(5), 1116–1124. https://doi.org/10.1161/01.cir.77.5.1116 |
| [14] | Peterzan MA, Lygate CA, Neubauer S, Rider O. Metabolic remodeling in hypertrophied and failing myocardium: a review. American Journal of Physiology. Heart and Circulatory Physiology, 2017; https://doi.org/10.1152/ajpheart.00731.2016 |
| [15] | Starling MR, Mancini GB, Montgomery DG, Gross MD. Relation between maximum time-varying elastance pressure-volume areas and myocardial oxygen consumption in dogs. Circulation 1991; Jan; 98(1): 304-14. https://doi.org/10.1161/01.cir.83.1.304 |
[1, 4, 5, 7-15]
. Chronic LL has been found to result with increased LV O₂ demand and early development of SD. However, when compared to EL there are studies showing that acute or chronic early LV load is related to early developing diastolic LV dysfunction and could be important as LL, resulting with SD
| [1] | Lam YY, Kaya MG, Li W, Gatzoulis MA, et al. Effect of Chronic Afterload Increase on Left Ventricular Myocardial Function in Patients With Congenital Left-Sided Obstructive Lesions Am J Cardiol 2007; 99: 1582–1587. |
| [13] | Nozawa T, Yasumura Y, Futaki S, Tanaka N, Uenishi M, Suga H. Efficiency of energy transfer from pressure-volume area to external mechanical work increases with contractile state and decreases with afterload in the left ventricle of the anesthetized closed-chest dog. Circulation, 1988; 77(5), 1116–1124. https://doi.org/10.1161/01.cir.77.5.1116 |
| [16] | Izzi G, Zile MR, Gaasch WH. Myocardial Oxygen Consumption and the Left Ventricular Pressure-Volume Area in Normal and Hypertrophic Canine Hearts. Circulation 1991; 84: 1384-1392. |
[1, 13, 16]
.
LV pressure-volume loop’s area represents the overall energy stored and released during mechanical contractions and is being considered to be a parameter for LV O₂ consumption
| [2] | Nozawa T, Yashumura Y, Futaka S, Tanaka N, Igarashi Y, et al. Relation between oxygen consumption and pressure-volume area of in situ dog heart. Am J Physiol 1987; 253: H31-H40. |
| [8] | Suga BH, Sagawa K. Instantaneous Pressure-Volume Relationships and Their Ratio in the Excised, Supported Canine Left Ventricle. Circulation Research, 1974; 35: 117–126. |
| [12] | Suga H, Hisano R, Hirata S, Hayashi T, Yamada O, Ninomiya I. Heart rate-independent energetics and systolic pressure-volume area in dog heart. Am J Physiol. 1983 Feb; 244(2): H206-14. https://doi.org/10.1152/ajpheart.1983.244.2.H206 |
| [15] | Starling MR, Mancini GB, Montgomery DG, Gross MD. Relation between maximum time-varying elastance pressure-volume areas and myocardial oxygen consumption in dogs. Circulation 1991; Jan; 98(1): 304-14. https://doi.org/10.1161/01.cir.83.1.304 |
[2, 8, 12, 15]
. This is important to determine LV functional capacity and reduce tolerance to increased LV load. Difference in LV pressure-volume area can be used to assess the LV mechanic work with O₂ demand in the development of insufficient systolic and diastolic LV function. In the presence of different LV loading, resulting from chronic early and late LV load, PVA, stroke work and EW with potential energy have not been assessed previously. This is needed in order to differentiate functional abnormalities early, including LV O₂ demand in LL and EL for early assessment of presence of diastolic and systolic LV dysfunction
| [2] | Nozawa T, Yashumura Y, Futaka S, Tanaka N, Igarashi Y, et al. Relation between oxygen consumption and pressure-volume area of in situ dog heart. Am J Physiol 1987; 253: H31-H40. |
| [20] | Parbhudayal R, Harms H, Mchels M, Van Rossum AC, Germans T, Van der Velden J. Increased myocardial oxygen consumption precedes contractile dysfunction in hypertrophic cardiomyopathy caused by pathogenic TNNT2 gene variants. J Am Heart Assoc. 2020; 9: e015316. https://doi.org/10.1161/JAHA.119.015316 |
| [21] | Laine H, Katoh C, Luotolahti M, Yki-Järvinen H, Kantola I, Jula A, et al. Myocardial oxygen consumption is unchanged but efficiency is reduced in patients with essential hypertension and left ventricular hypertrophy. Circulation. 1999; 100: 2425–2430. https://doi.org/10.1161/01.cir.100.24.2425 |
| [22] | Abou Ezzeddine OF, Kemp BJ, Borlaug BA et al, Myocardial Energetics in Heart Failure. Circ Heart Fail. 2019; 12: e006240. https://doi.org/10.1161/CIRCHEARTFAILURE.119.006240 |
| [23] | Bombardini T, Costantino MF, Sicari R, Ciampi Q, Pratali L, Picano E. End-Systolic Elastance and Ventricular-Arterial Coupling Reserve Predict Cardiac Events in Patients with Negative Stress Echocardiography. BioMed Research International, 2013, 1–14. https://doi.org/10.1155/2013/235194 |
[2, 20-23]
.
In order to assess energetic depth present within chronic LL vs. EL in early SD, the aim was to investigate whether defects in LV O₂ demand and stroke work are present in the 4th vs. 8th week period in the LV pressure-volume loop’s area. The hypothesis tested whether difference with imbalance between LV stroke work with PE and PV loop area for absolute O₂ demand are related to difference in load, comparing nonpulsatile with pulsatile LV afterload in porcine heart.
Increased LV pressure-volume loop’s area and stroke work are being described in arterial hypertension in the presence of LVH remodeling compared to normal left ventricles and in aortic stenosis in presence of symptoms, having reduced systolic LV function, as well as in chronic HF
| [10] | Hansson NH, Sörensen J, Harms HJ, Kim WY, Nielsen R, Tolbod LP, et al. Myocardial Oxygen Consumption and Efficiency in Aortic Valve Stenosis Patients With and Without Heart Failure. J Am Heart Assoc. 2017 Feb 6; 6(2): e004810. https://doi.org/10.1161/JAHA.116.004810 |
| [16] | Izzi G, Zile MR, Gaasch WH. Myocardial Oxygen Consumption and the Left Ventricular Pressure-Volume Area in Normal and Hypertrophic Canine Hearts. Circulation 1991; 84: 1384-1392. |
| [19] | Akinboboye OO, Chou RL, Bergmann SR. Myocardial blood flow and efficiency in concentric and eccentric left ventricular hypertrophy. American Journal of Hypertension, 2004; 17(5), 433–438. https://doi.org/10.1016/j.amjhyper.2004.02.006 |
| [20] | Parbhudayal R, Harms H, Mchels M, Van Rossum AC, Germans T, Van der Velden J. Increased myocardial oxygen consumption precedes contractile dysfunction in hypertrophic cardiomyopathy caused by pathogenic TNNT2 gene variants. J Am Heart Assoc. 2020; 9: e015316. https://doi.org/10.1161/JAHA.119.015316 |
| [21] | Laine H, Katoh C, Luotolahti M, Yki-Järvinen H, Kantola I, Jula A, et al. Myocardial oxygen consumption is unchanged but efficiency is reduced in patients with essential hypertension and left ventricular hypertrophy. Circulation. 1999; 100: 2425–2430. https://doi.org/10.1161/01.cir.100.24.2425 |
| [22] | Abou Ezzeddine OF, Kemp BJ, Borlaug BA et al, Myocardial Energetics in Heart Failure. Circ Heart Fail. 2019; 12: e006240. https://doi.org/10.1161/CIRCHEARTFAILURE.119.006240 |
| [23] | Bombardini T, Costantino MF, Sicari R, Ciampi Q, Pratali L, Picano E. End-Systolic Elastance and Ventricular-Arterial Coupling Reserve Predict Cardiac Events in Patients with Negative Stress Echocardiography. BioMed Research International, 2013, 1–14. https://doi.org/10.1155/2013/235194 |
| [24] | Kelly RP, Tunin R, Kass DA. Effect of Reduced Aortic Compliance on Cardiac Efficiency and Contractile Function of In Situ Canine Left Ventricle. Circ 1992; 71: 490–502. |
[10, 16, 19-24]
. However, a relative difference in LV pressure-volume loop’s area has not been assessed in association with the SD for difference in systolic LV load and its relation to normalized PVA per body surface area BSA (m²) and LVH remodeling (per 100 grams of LV mass) at 4
th vs 8
th week.
2. Methods
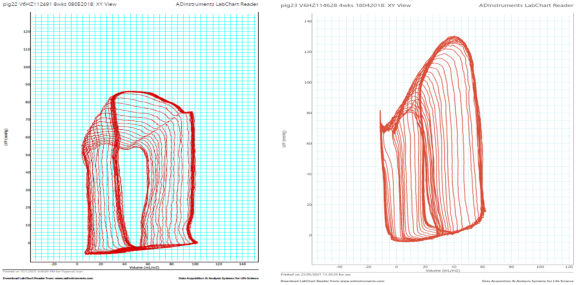
In fourteen domestic male pigs (28±3.4 kg) that underwent randomly either descending thoracic (n=8) or ascending aortic stenosis (n=6) during 8 weeks, LV invasive P-V loops’ were obtained during LV preload reduction, with inflating balloon catheter in inferior vena cava (
figure 1).
After sedation with intramuscular Telazol (Zoletil 100, 8mg/kg) and Xylazine M 2% (2.5mg/kg) for endotracheal intubation, anesthesia was induced intravenously (Propofol bolus dose 3 mg/kg). It was continued with intravenous combination of Propofol (10 mg/kg/h) and Fentanyl (18 µg/kg/h).
Mechanical ventilation maintained inspiratory 50% SaO₂ (Drager ventilator), with tidal volume 9-10 ml/kg; fr.16/min This kept arterial SaO₂ between 98-100 % and CO₂ under 35%. Intravenous NaCl 0.9% infusion (5-10 ml/kg/h) maintained a normal range of heart rate and blood pressure.
Following preparation with dissection of the common carotid artery and external jugular vein, with enoxaparin, administered intravenously for clot prevention (100 IU/kg), serial LV pressure-volume loops were obtained during afterload and preload reduction. This was recorded digitally in LabChart 7 (AD Instruments, Houston, Texas, USA, KU Leuven), having mechanical ventilation preserved and suspended transitionally, during preload reduction. For LV load reduction, inflating 10Fr balloon catheters was positioned in the inferior vena cava above the diaphragm, using guidewire.
The P-V catheter was calibrated at atmospheric pressure and we used manometer calibration within LabChart 7. LV volumes were assessed from cine cMRI LV volumes’ that were used. LV pressure-volume loops’ measurements were performed (Millar 5Fr pig-tailed conductance catheter) in the 4
th vs. 8
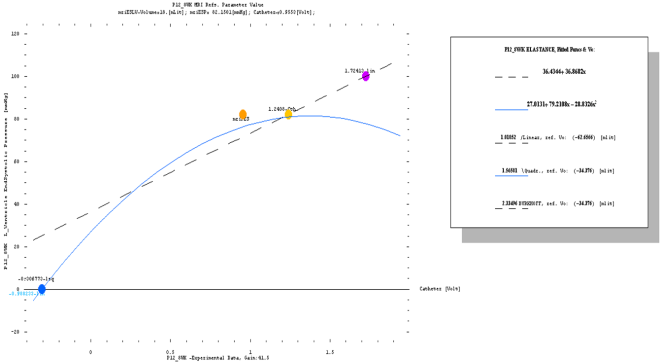
th weeks of surgical creation of moderate aortic stenosis. LV maximal end-systolic elastance was calculated, using special software and was used to assess the pressure-volume loop’s plane, from single nonlinear regression assessment (
figure 2). LV stroke work and pressure-volume area with effective work were analyzed, as parameters of systolic LV dysfunction, with maximum LV O₂ demand in different LV afterloads (late vs. early systolic LV load) between 4
th vs. 8
th week.
Figure 1. Presents LV P-V loops at maximal LV load reduction, with LV PVA in LL (up) vs. EL (down figure) in the 8th week.
LV stroke work and pressure-volume loop’s area were assessed, from the systolic part from the P-V loop and the LV O₂ demand in absolute and relative volumes, indexed per BSA and LV mass in different LV afterloads (late vs. early systolic LV load), so to characterize the LV work with O₂ demand, for SD assessment.
Stroke work and its index (SWI) were calculated as LV stroke volume (index) × end-systolic LV pressure. Maximal ESLVP was measured from the LV PV loop of single heart beat
| [2] | Nozawa T, Yashumura Y, Futaka S, Tanaka N, Igarashi Y, et al. Relation between oxygen consumption and pressure-volume area of in situ dog heart. Am J Physiol 1987; 253: H31-H40. |
| [3] | Loke KE, Messina EJ, Shesely EG. Et al. Potential role of eNOS in the therapeutic control of myocardial oxygen consumption by ACE inhibitors and amlodipine. Cardiovascular research 2001; 49(1), 86-93. https://doi.org/10.1016/S0008-6363(00)00196-6 |
[2, 3]
.
LV pressure-volume loops` area (PVA), an index of O₂ demand LVO₂, was calculated as SW and SWI + potential energy, being defined as: end-systolic LV pressure from the loop × (end-systolic volume (index) −Ves0)/2), having Ves0 be the volume-axis intercept of the nonlinear end-systolic pressure-volume relationship fit
| [6] | Burkhoff D, Yue DT, Oikawa RY, Franz MR, Schaefer J, Sagawa K. Influence of ventricular contractility on non-work-related myocardial oxygen consumption. Heart and Vessels, 1987; 3: 66–72. |
| [23] | Bombardini T, Costantino MF, Sicari R, Ciampi Q, Pratali L, Picano E. End-Systolic Elastance and Ventricular-Arterial Coupling Reserve Predict Cardiac Events in Patients with Negative Stress Echocardiography. BioMed Research International, 2013, 1–14. https://doi.org/10.1155/2013/235194 |
[6, 23]
. Maximum LV O₂ demand was assessed from the pressure-volume area and per heart beat, being presented in Joules.
Theoretical LV potential energy for LV volumes at end-systolic pressure of 100 mmHg (Ves100) from the nonlinear ESPVR regression was calculated from the LV P-V loops’ measurements in the 4th vs. 8th weeks.
CMRI measured end-systolic and end-diastolic LV volumes’ analysis was performed with software for cMRI images assessment (K.U. Leuven, CardioViewer). Left ventricular ESPVR and PVA parameters were further indexed, being assessed from LV volumes indexed per BSA (m2) and 100 grams of LV mass, that was measured from cine cMRIs.
For statistical analysis of variance in R studio, two-way repeated measures ANOVA with post hoc Tukey test were used, having p<0.05 considered as significant level. In addition, p<0.1 was consider for the post hoc analysis, with Levene normality test assessment. Analysis of the variance of aligned nonlinear transformation of the data was performed, as a nonparametric test.
Results are presented as means±SEM or medians with an interquartile range in the 4th vs. 8th week between chronic late and early loaded groups.
3. Results
The LV pressure-volume loop’s area being assessed in LL compares to EL in the 4
th vs. 8
th weeks of banding, with potential energy (PE), LVO₂ demands, LV stroke work, and effective work (EW) in absolute and relative values in terms of BSA are presented in detail in
table 1.
Normalization in terms of LV mass showed similar results when compare to BSA indexing of the nonlinear ESPVR curve.
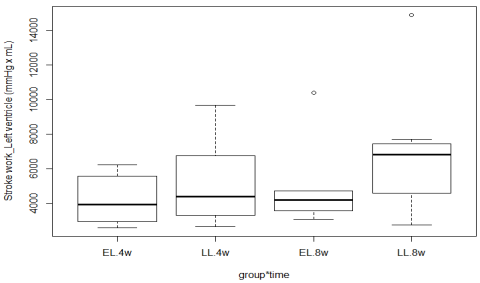
Stroke work was not different or changed between 4
th vs. 8
th week (
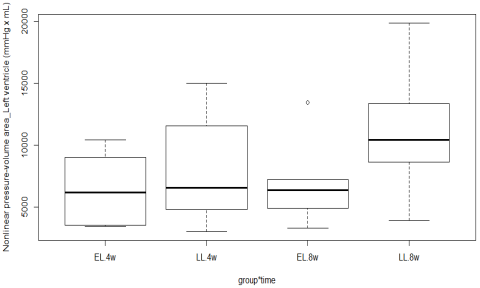
figure 3). LV PVA, with maximum LV O₂ demand, was also not different between groups, although being higher in LL compares to EL in the 8
th week. This was calculated using the nonlinear regression analysis of ESPVR (
figure 4).
Indexed LV stroke work for BSA (m²) and per 100 grams of LV mass were not different between LL and EL group. LV PVA was not different neither was changed significantly between groups, when indexed for m² BSA and per 100 grams of LV mass.
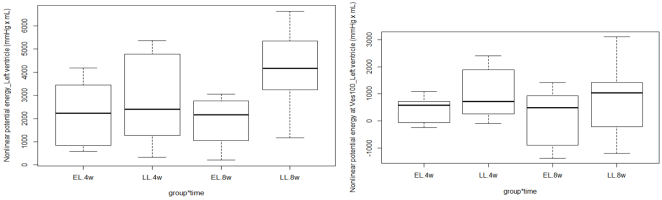
The potential LV energy in linear ESPVR (PE) was different. It trended to be associated with the LV systolic loading sequence, being higher in the LL compared with the EL group in the 8th week (interaction p=0.07). This was not found in PVA regression assessed, from maximum LV afterload in indexed LV volumes per m² BSA at 4th vs. 8th week.
Figure 2. Presents the software for nonlinear ESPVR assessment for PVA analysis in asc. banding (Pig12_8th week) with EL. It was performed, for nonlinear and linear regression, using absolute LV volumes. These were compared. The nonlinear ESPVR assessment of LV elastance with VA coupling is being discussed in other research article (unpublished data with results).
Table 1. Presenting LV PVA parameters, from ESPVR assessment using absolute and indexed LV volumes per BSA in m².
LV_PVA parameters | LL (n=8) 4th week | EL (n=6) 4th week | LL (n=8) 8th week | EL (n=6) 8th week | p group |
SW (mmHg·mL) | 5152±868 | 4209±600 | 6908±1287 | 5029±1097 | 0.5 |
SWi (mmHg·mL/m²) | 5072±669 | 4081±415 | 5797±833 | 3596±291 | 0.3 |
PE (mmHg·mL) | 2589 (1341-4580) | 2085 (1051-3278) | 3686 (3368-5180) | 1613 (1251-2691) | 0.5 |
PEi mmHg·mL/m² | 2734±567 | 3612±1367 | 3161 (1963-4251) | 1698±351 | 0.6 |
PE100 (mmxHg·mL) | 1008±337 | 446±205 | 802±488 | 177±443 | 0.3 |
PVA (mmHg·mL) | 7817±1587 | 6527±1102 | 10482±1609 | 5389±583 | 0.5 |
PVAi (mmHg·mL/m²) | 7806±949 | 7693±1660 | 9527 (7015-10821) | 5294±513 | 0.7 |
LVO₂ (J/min) | 1.1±0.2 | 0.86±0.16 | 1.5±0.2 | 0.9±0.2 | 0.5 |
LVO₂i (J/min/m²) | 1.04±0.1 | 1 ±0.2 | 1.2 (0.92-1.44) | 0.7±0.07 | 0.7 |
LVO₂I (J/beat/m²) | 0.013±0.002 | 0.014±0.003 | 0.014 (0.01-0.185) | 0.01±0.0013 | 0.8 |
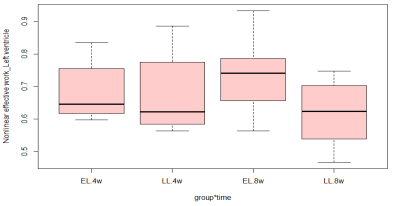
EW | 0.69±0.04 | 0.65±0.03 | 0.63±0.03 | 0.74±0.05 | 0.39 |
EWi | 0.66±0.05 | 0.6±0.07 | 0.6 (0.55-0.74) | 0.7±0.05 | 0.96 |
TABLE legends: SW –stroke work, PE potential energy, PVA for PV area, EW for effective work. LVO₂ for nonlinear analysis of LV O₂ demand, (LVO₂=PVA*1, 33*10^-4 Nozawa et al -reff. list), † for p<0.05 in two-way repeated measurement ANOVA for group difference; ¶ for significant interaction effect; $ for significant change between 4th vs. 8th week.
Figure 3. Presents the LV stroke work in LL vs. EL group - no significant difference was found between the groups or change at 4th & 8th week.
Figure 4. Left ventricular pressure-volume area was calculated using the nonlinear ESPVR regression method, in LL and EL presents no significant difference at 4th or 8th week.
Nonlinear ESPVR analysis did not present difference in the nonlinear potential LV energy (PEb) in LL compares to EL, neither change from the systolic LV load between 4
th vs. 8
th week (
figure 5). This was also found when ESPVR was assessed from indexed LV volumes per BSA and per 100 grams of LV mass. The theoretical LV potential energy for ventricular volume at 100 mmHg end-systolic LV pressure was not different significantly, when being assessed from nonlinear regression method. It was higher in LL compared to EL in hypertrophic LV remodeling presented per 100 grams of LV mass in the 8
th week (post hoc p=0.036).
LV O₂ demand was not different, though being higher in LL at 8th week (LVO₂b in LL 4 weeks 0.013±0.003 and 8 weeks 0.018±0.002 J/beat vs. EL 4weeks 0.011±0.003 and 8 week 0.01±0.0015 J/beat p=0.04 group). There were no differences for indexed LV O₂ demand between LL and EL group in the 4th vs. 8th week.
LV PVA was not different between LL and EL indexed per BSA, and when assessed in 100gr LV mass for LVH remodeling. Effective LV work was also not different neither changed, being reduced in LL compared to the EL group between 4
th vs. 8
th week (
figure 6).
This was result from difference in LV afterload.
Figure 5. Showing no difference for LV ventricular potential energy, calculated using the nonlinear regression method in the 8th week. Nonlinear potential energy at Ves100 was not different in LL compares to EL between 4th vs. 8th week.
Figure 6. Effective LV work assessed, using the nonlinear regression method for ESPVR assessment, is not different in different systolic LV load comparing LL with EL in the 4th vs. 8th week.
4. Discussion
This study that assessed in LVH, both relative and absolute LV SW with maximum O₂ demand from the pressure-volume loop’s area, with EW, showed no differences in LV potential energy or absolute LV O₂ demand and systolic dysfunction, as well as from normalized effective LV work, having no changes in chronic LL and EL between 4
th vs. 8
th week. Differences were present, being found previously in LL vs. EL
| [13] | Nozawa T, Yasumura Y, Futaki S, Tanaka N, Uenishi M, Suga H. Efficiency of energy transfer from pressure-volume area to external mechanical work increases with contractile state and decreases with afterload in the left ventricle of the anesthetized closed-chest dog. Circulation, 1988; 77(5), 1116–1124. https://doi.org/10.1161/01.cir.77.5.1116 |
| [19] | Akinboboye OO, Chou RL, Bergmann SR. Myocardial blood flow and efficiency in concentric and eccentric left ventricular hypertrophy. American Journal of Hypertension, 2004; 17(5), 433–438. https://doi.org/10.1016/j.amjhyper.2004.02.006 |
| [21] | Laine H, Katoh C, Luotolahti M, Yki-Järvinen H, Kantola I, Jula A, et al. Myocardial oxygen consumption is unchanged but efficiency is reduced in patients with essential hypertension and left ventricular hypertrophy. Circulation. 1999; 100: 2425–2430. https://doi.org/10.1161/01.cir.100.24.2425 |
| [22] | Abou Ezzeddine OF, Kemp BJ, Borlaug BA et al, Myocardial Energetics in Heart Failure. Circ Heart Fail. 2019; 12: e006240. https://doi.org/10.1161/CIRCHEARTFAILURE.119.006240 |
[13, 19, 21, 22]
. Furthermore, indexing PVA parameters did not find difference, being relevant and related to EL and LL group in the 4
th or 8
th week. These relevant findings show no difference in SD from LV nonlinear pressure-volume loop’s area assessment when maximal end-systolic LV elastance is used to calculate the O₂ demand in LL and EL. It further indicates no difference in increased LV O₂ demand between chronic LL and EL in the 8
th week.
Increased LV O₂ demands and reduced EW are related to the increased afterload, in earlier developmental reduction in contractile LV function, as found in LL compared to EL group, with further developing earlier chronic systolic in diastolic LV dysfunction and decompensated stage of LVH remodeling
. However, the most important finding of this study is that in EL vs LL there is no difference in stroke work and effective work at 4
th and 8
th week, in PVA plane assessment in SD, being present.
In this porcine model of chronic LL to compare with EL, there was no difference in LV mass, being calculated from cMRI, except in RWT in the 8
th week, presenting with thicker concentric LVH in EL (DB 0.45 vs. AB 0.67 p=0.003)
| [17] | Popevska S., et al. Adverse left ventricular hypertrophy in descending thoracic vs. ascending aorta banding in novel porcine model. cMRI study. Presented abstract ESC 2019 poster presented in Paris France, published in European Heart Journal (2019), 40 Supplement, 911. |
| [18] | Popevska S et al. Different left ventricular remodeling between descending thoracic vs. ascending aorta banding in porcine model. Abstract presentation ESCVS 2019 Groningen NL. published in Journal of Cardiovascular Surgery 2019; Vol 60, Suppl. 1 to No3.: 401, 56. |
[17, 18]
. Concentric LVH remodeling in arterial hypertension or AS is related to reduced mechanical myocardial work compared to eccentric LVH remodeling, resulting from differences present in LV stroke work and reduced O₂ extraction, within increased demand having worsen SD
| [10] | Hansson NH, Sörensen J, Harms HJ, Kim WY, Nielsen R, Tolbod LP, et al. Myocardial Oxygen Consumption and Efficiency in Aortic Valve Stenosis Patients With and Without Heart Failure. J Am Heart Assoc. 2017 Feb 6; 6(2): e004810. https://doi.org/10.1161/JAHA.116.004810 |
| [19] | Akinboboye OO, Chou RL, Bergmann SR. Myocardial blood flow and efficiency in concentric and eccentric left ventricular hypertrophy. American Journal of Hypertension, 2004; 17(5), 433–438. https://doi.org/10.1016/j.amjhyper.2004.02.006 |
[10, 19]
. In this study, difference present in LVH remodeling for the LV relative wall thickness did not present difference in effective LV work between groups in the 4
th or 8
th week and when being indexed, also per LV mass.
In previous report, assessing the PVA in increased LV afterload for early SD showed increased PVA with reduced effective LV work
| [13] | Nozawa T, Yasumura Y, Futaki S, Tanaka N, Uenishi M, Suga H. Efficiency of energy transfer from pressure-volume area to external mechanical work increases with contractile state and decreases with afterload in the left ventricle of the anesthetized closed-chest dog. Circulation, 1988; 77(5), 1116–1124. https://doi.org/10.1161/01.cir.77.5.1116 |
| [21] | Laine H, Katoh C, Luotolahti M, Yki-Järvinen H, Kantola I, Jula A, et al. Myocardial oxygen consumption is unchanged but efficiency is reduced in patients with essential hypertension and left ventricular hypertrophy. Circulation. 1999; 100: 2425–2430. https://doi.org/10.1161/01.cir.100.24.2425 |
[13, 21]
. This is related to reduced O₂ extraction level in higher LV working state and increased LV load
| [22] | Abou Ezzeddine OF, Kemp BJ, Borlaug BA et al, Myocardial Energetics in Heart Failure. Circ Heart Fail. 2019; 12: e006240. https://doi.org/10.1161/CIRCHEARTFAILURE.119.006240 |
| [23] | Bombardini T, Costantino MF, Sicari R, Ciampi Q, Pratali L, Picano E. End-Systolic Elastance and Ventricular-Arterial Coupling Reserve Predict Cardiac Events in Patients with Negative Stress Echocardiography. BioMed Research International, 2013, 1–14. https://doi.org/10.1155/2013/235194 |
| [24] | Kelly RP, Tunin R, Kass DA. Effect of Reduced Aortic Compliance on Cardiac Efficiency and Contractile Function of In Situ Canine Left Ventricle. Circ 1992; 71: 490–502. |
| [25] | Bachte R, Zheng Dai X. Myocardial oxygen consumption during exercise in the presence of left ventricular hypertrophy secondary to supravalvular aortic stenosis. JACC 1990; 5(15): 1157-64. |
[22-25]
.
In increased LV afterload, the LV hypertrophy and development of SD has been related to imbalance between the intraventricular coupling, the LV working range and energy potentials, resulting with increased LVO₂ demands at rest.
These relative findings indicate indexed PVA parameters of the end-systolic pressure-volume relation for BSA and per 100 grams LV mass, as parameters for LV O₂ demand are not different, in LL vs. EL group in the 4th vs. 8th week. This did not change in LL or EL.
The coupling between the LV contractility and the LV afterload have been extensively evaluated in previous studies showing that, in physiologic condition, there is an adaptation to differences for the peak in LV afterload
| [2] | Nozawa T, Yashumura Y, Futaka S, Tanaka N, Igarashi Y, et al. Relation between oxygen consumption and pressure-volume area of in situ dog heart. Am J Physiol 1987; 253: H31-H40. |
| [5] | Burkhoff D, Sagawa K. Ventricular efficiency predicted by an analytical model. The American Journal of Physiology, 1986; 250(6): R1021–R1027. |
| [8] | Suga BH, Sagawa K. Instantaneous Pressure-Volume Relationships and Their Ratio in the Excised, Supported Canine Left Ventricle. Circulation Research, 1974; 35: 117–126. |
| [13] | Nozawa T, Yasumura Y, Futaki S, Tanaka N, Uenishi M, Suga H. Efficiency of energy transfer from pressure-volume area to external mechanical work increases with contractile state and decreases with afterload in the left ventricle of the anesthetized closed-chest dog. Circulation, 1988; 77(5), 1116–1124. https://doi.org/10.1161/01.cir.77.5.1116 |
| [15] | Starling MR, Mancini GB, Montgomery DG, Gross MD. Relation between maximum time-varying elastance pressure-volume areas and myocardial oxygen consumption in dogs. Circulation 1991; Jan; 98(1): 304-14. https://doi.org/10.1161/01.cir.83.1.304 |
[2, 5, 8, 13, 15]
. However, ability to tolerate stress in the intraventricular coupling assessed through the pressure-volume loop’s area analysis is not precisely defined in chronic LL and EL in developing systolic with diastolic LV dysfunction
| [1] | Lam YY, Kaya MG, Li W, Gatzoulis MA, et al. Effect of Chronic Afterload Increase on Left Ventricular Myocardial Function in Patients With Congenital Left-Sided Obstructive Lesions Am J Cardiol 2007; 99: 1582–1587. |
| [5] | Burkhoff D, Sagawa K. Ventricular efficiency predicted by an analytical model. The American Journal of Physiology, 1986; 250(6): R1021–R1027. |
| [19] | Akinboboye OO, Chou RL, Bergmann SR. Myocardial blood flow and efficiency in concentric and eccentric left ventricular hypertrophy. American Journal of Hypertension, 2004; 17(5), 433–438. https://doi.org/10.1016/j.amjhyper.2004.02.006 |
| [21] | Laine H, Katoh C, Luotolahti M, Yki-Järvinen H, Kantola I, Jula A, et al. Myocardial oxygen consumption is unchanged but efficiency is reduced in patients with essential hypertension and left ventricular hypertrophy. Circulation. 1999; 100: 2425–2430. https://doi.org/10.1161/01.cir.100.24.2425 |
| [22] | Abou Ezzeddine OF, Kemp BJ, Borlaug BA et al, Myocardial Energetics in Heart Failure. Circ Heart Fail. 2019; 12: e006240. https://doi.org/10.1161/CIRCHEARTFAILURE.119.006240 |
[1, 5, 19, 21, 22]
.
Indexed LVO₂ demand was reported as not different between hypertrophic and normal LVs. However, it was different, when using absolute volumes, thereby indicating the impact of LV mass being present on basal resting O₂ demand
| [16] | Izzi G, Zile MR, Gaasch WH. Myocardial Oxygen Consumption and the Left Ventricular Pressure-Volume Area in Normal and Hypertrophic Canine Hearts. Circulation 1991; 84: 1384-1392. |
[16]
. This is somehow related to LV stroke work in HTA
| [25] | Bachte R, Zheng Dai X. Myocardial oxygen consumption during exercise in the presence of left ventricular hypertrophy secondary to supravalvular aortic stenosis. JACC 1990; 5(15): 1157-64. |
[25]
. Further, imbalances in LV mechanical effective work have been associated with the presence of LVH, being present in arterial hypertension
| [21] | Laine H, Katoh C, Luotolahti M, Yki-Järvinen H, Kantola I, Jula A, et al. Myocardial oxygen consumption is unchanged but efficiency is reduced in patients with essential hypertension and left ventricular hypertrophy. Circulation. 1999; 100: 2425–2430. https://doi.org/10.1161/01.cir.100.24.2425 |
[21]
.
Ventricular contractility and myocardial O₂ consumption are coupled closely in the ventricles and the heart, being heart rate dependent, in both physiological and pathological conditions
| [8] | Suga BH, Sagawa K. Instantaneous Pressure-Volume Relationships and Their Ratio in the Excised, Supported Canine Left Ventricle. Circulation Research, 1974; 35: 117–126. |
| [9] | Suga H, Sagawa K, Shoukas AA. Load independence of the instantaneous pressure-volume ratio of the canine left ventricle and effects of epinephrine and heart rate on the ratio. Circ Res. 1973; 32(3): 314-322. https://doi.org/10.1161/01.res.32.3.314 |
| [12] | Suga H, Hisano R, Hirata S, Hayashi T, Yamada O, Ninomiya I. Heart rate-independent energetics and systolic pressure-volume area in dog heart. Am J Physiol. 1983 Feb; 244(2): H206-14. https://doi.org/10.1152/ajpheart.1983.244.2.H206 |
[8, 9, 12]
. However, in diastolic LV dysfunction and in HF there is an inadequate response to stress and resting state in heart rate that can have an impact on the resting LV working state. These relative changes may present earlier affection of LV O₂ demand, being increased at rest and worsen with stress earlier before systolic LV function would present its fall in effective end-systolic LV elastance.
Further metabolic changes of the LV myocardium are earlier LV changes in its shape and structure, changes that have not been analyzed in vivo for the non–working related LV myocardium
| [21] | Laine H, Katoh C, Luotolahti M, Yki-Järvinen H, Kantola I, Jula A, et al. Myocardial oxygen consumption is unchanged but efficiency is reduced in patients with essential hypertension and left ventricular hypertrophy. Circulation. 1999; 100: 2425–2430. https://doi.org/10.1161/01.cir.100.24.2425 |
[21]
. It was showed that non-indexed myocardial O₂ consumption is greater in LVH and has been related to the extent of the LV mass, correlating inversely with mechanical myocardial efficiency in several reports
| [16] | Izzi G, Zile MR, Gaasch WH. Myocardial Oxygen Consumption and the Left Ventricular Pressure-Volume Area in Normal and Hypertrophic Canine Hearts. Circulation 1991; 84: 1384-1392. |
| [21] | Laine H, Katoh C, Luotolahti M, Yki-Järvinen H, Kantola I, Jula A, et al. Myocardial oxygen consumption is unchanged but efficiency is reduced in patients with essential hypertension and left ventricular hypertrophy. Circulation. 1999; 100: 2425–2430. https://doi.org/10.1161/01.cir.100.24.2425 |
| [22] | Abou Ezzeddine OF, Kemp BJ, Borlaug BA et al, Myocardial Energetics in Heart Failure. Circ Heart Fail. 2019; 12: e006240. https://doi.org/10.1161/CIRCHEARTFAILURE.119.006240 |
| [23] | Bombardini T, Costantino MF, Sicari R, Ciampi Q, Pratali L, Picano E. End-Systolic Elastance and Ventricular-Arterial Coupling Reserve Predict Cardiac Events in Patients with Negative Stress Echocardiography. BioMed Research International, 2013, 1–14. https://doi.org/10.1155/2013/235194 |
[16, 21-23]
. Shift of contractility in the PVA plane may case linear parallel shift in basal non-work related myocardial O₂ consumed for 100 grams in LV mass in situ, where ESPVR may become more or less linear in presence of LVH remodeling
| [5] | Burkhoff D, Sagawa K. Ventricular efficiency predicted by an analytical model. The American Journal of Physiology, 1986; 250(6): R1021–R1027. |
| [6] | Burkhoff D, Yue DT, Oikawa RY, Franz MR, Schaefer J, Sagawa K. Influence of ventricular contractility on non-work-related myocardial oxygen consumption. Heart and Vessels, 1987; 3: 66–72. |
[5, 6]
.
In TNNT2 cardiomyopathy or in HTA and AS, systolic LV dysfunction in LVH remodeling, having positive genotype with phenotype negative feature presenting absent LV hypertrophic remodeling in the progression towards HF with contractile dysfunction has increased LV O₂ consumption with reduced mechanical myocardial efficiency
| [19] | Akinboboye OO, Chou RL, Bergmann SR. Myocardial blood flow and efficiency in concentric and eccentric left ventricular hypertrophy. American Journal of Hypertension, 2004; 17(5), 433–438. https://doi.org/10.1016/j.amjhyper.2004.02.006 |
| [20] | Parbhudayal R, Harms H, Mchels M, Van Rossum AC, Germans T, Van der Velden J. Increased myocardial oxygen consumption precedes contractile dysfunction in hypertrophic cardiomyopathy caused by pathogenic TNNT2 gene variants. J Am Heart Assoc. 2020; 9: e015316. https://doi.org/10.1161/JAHA.119.015316 |
| [22] | Abou Ezzeddine OF, Kemp BJ, Borlaug BA et al, Myocardial Energetics in Heart Failure. Circ Heart Fail. 2019; 12: e006240. https://doi.org/10.1161/CIRCHEARTFAILURE.119.006240 |
| [25] | Bachte R, Zheng Dai X. Myocardial oxygen consumption during exercise in the presence of left ventricular hypertrophy secondary to supravalvular aortic stenosis. JACC 1990; 5(15): 1157-64. |
[19, 20, 22, 25]
. However, presence of LVH is important for reduced ability to tolerate exercise or stress, being result of SD
| [1] | Lam YY, Kaya MG, Li W, Gatzoulis MA, et al. Effect of Chronic Afterload Increase on Left Ventricular Myocardial Function in Patients With Congenital Left-Sided Obstructive Lesions Am J Cardiol 2007; 99: 1582–1587. |
| [21] | Laine H, Katoh C, Luotolahti M, Yki-Järvinen H, Kantola I, Jula A, et al. Myocardial oxygen consumption is unchanged but efficiency is reduced in patients with essential hypertension and left ventricular hypertrophy. Circulation. 1999; 100: 2425–2430. https://doi.org/10.1161/01.cir.100.24.2425 |
| [24] | Kelly RP, Tunin R, Kass DA. Effect of Reduced Aortic Compliance on Cardiac Efficiency and Contractile Function of In Situ Canine Left Ventricle. Circ 1992; 71: 490–502. |
[1, 21, 24]
.
There are different phenotypes of metabolic changes of the LV myocardium that are related to the phase of the hypertrophic ventricular remodeling when being assessed that is also related to the NYHA class and EF
| [10] | Hansson NH, Sörensen J, Harms HJ, Kim WY, Nielsen R, Tolbod LP, et al. Myocardial Oxygen Consumption and Efficiency in Aortic Valve Stenosis Patients With and Without Heart Failure. J Am Heart Assoc. 2017 Feb 6; 6(2): e004810. https://doi.org/10.1161/JAHA.116.004810 |
| [14] | Peterzan MA, Lygate CA, Neubauer S, Rider O. Metabolic remodeling in hypertrophied and failing myocardium: a review. American Journal of Physiology. Heart and Circulatory Physiology, 2017; https://doi.org/10.1152/ajpheart.00731.2016 |
| [21] | Laine H, Katoh C, Luotolahti M, Yki-Järvinen H, Kantola I, Jula A, et al. Myocardial oxygen consumption is unchanged but efficiency is reduced in patients with essential hypertension and left ventricular hypertrophy. Circulation. 1999; 100: 2425–2430. https://doi.org/10.1161/01.cir.100.24.2425 |
| [22] | Abou Ezzeddine OF, Kemp BJ, Borlaug BA et al, Myocardial Energetics in Heart Failure. Circ Heart Fail. 2019; 12: e006240. https://doi.org/10.1161/CIRCHEARTFAILURE.119.006240 |
[10, 14, 21, 22]
.
In this report, it was shown that absolute LV O₂ demand and LV potential energy with stroke work are not different or affected in LL and EL and are different compares to ventricular arrhythmia occurrence group. LV stroke work was not different between these two groups, being higher in LL compares with EL. These differences were not significant in the 8th week and when PVA parameters were indexed per 100 grams of LV mass or BSA. However, difference was found in LV nonlinear PE for 100 mmHg end-systolic pressures when indexed per 100 grams LV mass.
Comparing LL to EL it was showed that the LV working range and limited LV ESPVR are different, being less in EL group when volumes for end-systolic pressure of 100 mmHg has been generated in both absolute or normalized PVA per 100 grams of LV mass. This is seen from the differences created in LV afterload that is relevant to understand why LVH remodeling with systolic dysfunction and insufficient filling can result especially from LL and in the 8
th week for EL. The most important finding of this study shows that PVA, as parameter of maximal LV O₂ demand during rest is not different between LL and EL with LV stroke work and effective work in the progression towards systolic HF, assessing metabolic remodeling. In previous findings it was showed how reduced aortic compliance, as well as presence of LVH in AS are related to increased MVO₂ consumption with demand of more that 30-50% compared from rest state. In HTA however, LVO₂ demand at peak exercise is reduced compares to controls, indicating reduced exercise capacity, due to higher heart rate and reduced vasodilator reserve with response to stress
| [22] | Abou Ezzeddine OF, Kemp BJ, Borlaug BA et al, Myocardial Energetics in Heart Failure. Circ Heart Fail. 2019; 12: e006240. https://doi.org/10.1161/CIRCHEARTFAILURE.119.006240 |
| [23] | Bombardini T, Costantino MF, Sicari R, Ciampi Q, Pratali L, Picano E. End-Systolic Elastance and Ventricular-Arterial Coupling Reserve Predict Cardiac Events in Patients with Negative Stress Echocardiography. BioMed Research International, 2013, 1–14. https://doi.org/10.1155/2013/235194 |
| [24] | Kelly RP, Tunin R, Kass DA. Effect of Reduced Aortic Compliance on Cardiac Efficiency and Contractile Function of In Situ Canine Left Ventricle. Circ 1992; 71: 490–502. |
| [25] | Bachte R, Zheng Dai X. Myocardial oxygen consumption during exercise in the presence of left ventricular hypertrophy secondary to supravalvular aortic stenosis. JACC 1990; 5(15): 1157-64. |
[22-25]
.
This novel and relevant finding indicates no difference present in LV stroke work and PVA earlier on between chronic LL and EL in the 4th vs. 8th week. There were no differences related with the LV hypertrophy developed, that was not different between LL and EL group or when normalized per BSA in the 4th vs. 8th week. These findings show that these are no differences being related to that associate with maximal absolute LV O₂ demand, at rest in EL and LL in the 4th and 8th week. LV potential energy, being stored during systole, was not different in this analysis, except for the nonlinear potential energy for Ves100 indexed for BSA, as for LV mass.
It was showed that presence of negative external LV work is related to the adaptive physiologic response of the ventricle
| [11] | Suga H, Goto Y, Yasumura Y, Nozawa T, Futaki S, Tanaka N, Uenishi M. Oxygen-saving effect of negative work in dog left ventricle. American Journal of Physiology-Heart and Circulatory Physiology, 1988; 254(1), H34–H44. https://doi.org/10.1152/ajpheart.1988.254.1.H34 |
[11]
. This was present in EL in this porcine model, indicating early SD in increased LV afterload. By comparison, in LL there was higher LV stroke work, presenting a more positive LV effective work for both Ves0 and Ves100, thus indicating that the ventricle is deteriorating by failing to generate negative effective stroke work. The novelty introduced in this study brings the value of intraventricular coupling, being assessed through the PVA, as relevant for differences in systolic LV loading, as found in the presence of arterial hypertension, coarctation or aortic stenosis in the development of earlier LV insufficient pump function, resulting from dysfunction of LV filling. Furthermore, the increased absolute LVO₂ demand in LL compared to EL can imply on the pathophysiologic background for developing earlier systolic or/and diastolic LV dysfunction, in LL or EL, being assessed previously
| [17] | Popevska S., et al. Adverse left ventricular hypertrophy in descending thoracic vs. ascending aorta banding in novel porcine model. cMRI study. Presented abstract ESC 2019 poster presented in Paris France, published in European Heart Journal (2019), 40 Supplement, 911. |
[17]
. This can be found in relation to ventricular arrhythmia occurrence. In this study LVEF was not different between groups in the 8
th week and there was no difference in PVA and LV O₂ demand, as well as in normalized PVA parameters in the 8
th week, except in PE for PES100. This was showed that can be assessed, from nonlinear regression assessment of ELV, indicating of early increased PE needed to complete LV relaxation in LL competed to EL, where is incomplete.
This is indirect parameter that may show reduced exercise capacity with increased resting LVO₂ demand, as relevant for different LV afterload, result of arterial hypertension.In the presence of aortic valve stenosis, reduced myocardial effective work with stroke work, and their blunt or reduced reserves at rest have been associated with presence of chronic systolic HF and higher NYHA functional class, suggesting on need of O₂ supplement in this condition
| [10] | Hansson NH, Sörensen J, Harms HJ, Kim WY, Nielsen R, Tolbod LP, et al. Myocardial Oxygen Consumption and Efficiency in Aortic Valve Stenosis Patients With and Without Heart Failure. J Am Heart Assoc. 2017 Feb 6; 6(2): e004810. https://doi.org/10.1161/JAHA.116.004810 |
[10]
. Though values of myocardial O₂ demand and stroke work are compared on individual bases, these present findings in this porcine model are representative for human pathophysiology, having thus comparable ventricular volumes, in moderate descending thoracic vs. ascending aortic stenosis resulting for differences in LV systolic load (timing and LVESP). Difference in pathology makes these different diseases different to compare and to assess nonpulsatile vs. pulsatile component of the LV afterload. This may be considered as range, in hypertension, (supracoronary) aortic stenosis and/or descending thoracic aorta stenosis associated with coarctation of the aorta being relevant for early SD. These several pathologic disease conditions promote the LVH remodeling processes, thereby affecting the ventricle with resulting changes of the LV with atrial shape, structure, and function, further leading towards development of LV relaxation abnormality and SD in increased load. This occurs within the hypertrophic and structurally changed ventricles, as a result of the afterload-related injury, promoting neurohormones and mechanical processes that affect the LV hypertrophic myocardium in terms of change in the metabolic substrate being used to complete LV relaxation.
In HF, mechanical myocardial efficiency is reduced with state of increased O₂ consumption by the LV myocardium, being reported in previous work
| [22] | Abou Ezzeddine OF, Kemp BJ, Borlaug BA et al, Myocardial Energetics in Heart Failure. Circ Heart Fail. 2019; 12: e006240. https://doi.org/10.1161/CIRCHEARTFAILURE.119.006240 |
| [23] | Bombardini T, Costantino MF, Sicari R, Ciampi Q, Pratali L, Picano E. End-Systolic Elastance and Ventricular-Arterial Coupling Reserve Predict Cardiac Events in Patients with Negative Stress Echocardiography. BioMed Research International, 2013, 1–14. https://doi.org/10.1155/2013/235194 |
[22, 23]
. Contractile LV deterioration in cardiomyopathy is related to an increased myocardial O₂ consumption of the septum with reduced effective work. In this model, the aim was to assess early systolic in diastolic LV dysfunction, from the myocardial effective work with O₂ demand. Instead, the assessment of stroke LV work through the PVA analysis found no difference in LL vs. EL group in systolic dysfunction from portion of PVA in the 4
th vs. 8
th week, when using maximal ELV for calculation of the PVA and maximum LV O₂ demand. LV stroke work reduced in EL compares to LL at 8
th week, showing that SD is more severe in EL vs. LL.
LV work with pressure-volume area calculation, from the pressure-volume loops, was performed based on maximum single end-systolic LV pressure measurement in normal heat beat to calculate the LV pressure-volume loop’s area, having the highest value from the pressure-volume measurement analyzed. The values were compared to multiples beats assessment that did not show difference. This method used for interpreting the invasive assessment of LV mechanical coupling, for assessing the diastolic and systolic function with their interaction are measurements of the LV work and efficiency, so to assess early SD and HF development. This kind of data interpretation is preferred in terms of better independent LV functional and energetic assessment for avoiding other relevant cardiovascular conditions that can affect the interpretation of the pressure-volume loop’s hysteresis when assessing the LV work and energetic potential with systolic-diastolic functional coupling in the PVA plane assessment.
In conclusion, absolute LV potential energy at Pes0, and LVO₂ demand are not different, as well as, stroke work and PVA with effective work in a model comparing LL and EL. Indexed LV PVA parameters for m² and per 100 grams of LV mass are not different between 4th vs. 8th week in LL compares to EL. This is cause for the development of earlier diastolic with systolic dysfunction in chronic LV afterload increase. This study found that LL is important for early systolic LV dysfunction, as well as EL having diastolic LV dysfunction.
Limitation of this study is the use of porcine model and need to compare these findings to previous dogs model that do not have the same anatomy and hemodynamic to be compared, as human. The baseline with resting basal LV O₂ demand have not been measured and calculated, limiting the present assessment.
Clinical perspective: in hypertensive model having increased LV load, LV stroke work with PVA and EW are not different, and PE with maximum LVO₂ demand at rest, during load reduction in LVH remodeling for early SD between 4th vs. 8th week. In HTA /AS model having LL and EL, nonlinear PVA parameters indicate that chronic LL compares to EL are both important for early development SD and HF, but earlier in EL. Difference found for PE100 indicates on relaxation changes in relation to intraventricular coupling relation, in assessment of early SD development in LL and EL.
Central message: No difference in SD is found presenting with LV SW with PVA and EW that are not different in nonlinear ESPVR regression, between LL and EL in the 4th vs. 8th week. Normalizing PVA for BSA in m² or per LV mass did not show different or was related to changes with differences in PE, when assessing early HF with SD, from P-V assessment of LV stroke work with maximum LV O₂ demand and EW, between 4th vs. 8th week in concentric LVH remodeling.